An Urgent Call for Change
Note: This report details traumatic and disturbing experiences of people subjected to involuntary commitment
Introduction
News of North Carolina’s mental health crisis is everywhere. More children and adults than ever need access to mental health services. In many cases, services don’t exist where people live or aren’t available when they desperately need them. Our people, and the system they rely on, are in crisis.
In desperation to get help, a loved one, friend, colleague, law enforcement officer, or mental health worker may seek involuntary commitment (IVC) for a child or adult. IVC is a forced treatment measure that should only be used as a last resort. As a society, many of us assume this is what should happen to keep the person and/or other people safe. Culturally, there is an unfortunate presumption that this is in the best interest of the person.
But what really happens when a person is involuntarily committed in North Carolina?
For more than a year, Disability Rights North Carolina (DRNC) focused intensively on NC’s IVC process and how it plays out on the ground. Using DRNC’s federally-mandated access authority[1], DRNC staff monitored emergency departments (EDs) across the state and interviewed people with lived experience and their families directly affected by IVC, as well as hospital officials, mental health advocates, and legal scholars.
What emerged is an overwhelmed mental health system where people of all ages, with serious behavioral health needs, languish in EDs without court-appointed legal counsel or adequate mental health treatment. The IVC process in NC begins after a magistrate signs a “custody order,” a civil, not criminal, order authorizing law enforcement agencies to detain and transport a person to a hospital. Once detained in an ED, the child or adult who is the focus of that order cannot leave; their liberty is quite literally in legal limbo because the law does not provide for an attorney or hearing in the ED.
Forced detention in an ED can last for days, weeks, and even months while awaiting an available bed for psychiatric hospitalization (commonly referred to as “ED boarding”). Once a bed is identified, often hours from home, the child or adult is transported to what is known as a “24-hour facility,” meaning a facility the NC Department of Health and Human Services (NC DHHS) designates for the custody and treatment of people in the IVC process.
It is at the 24-hour facility that NC law finally provides the first glimpse of due process, allowing for the appointment of an attorney and a right to appear at an IVC hearing before a judge. By law, this hearing must occur within 10 days after the individual is detained.
At this “commitment hearing,” the first legally required court hearing since the individual was forcibly detained, a district court judge determines if the person should be involuntarily committed. If that occurs, the IVC designation will be recorded in court files and will present lifelong obstacles regardless of treatment compliance, efficacy, or outcomes.
NC collects very little data about the IVC process, so it is difficult to fully analyze where adjustments to law or policy should be made to prevent its wrongful, wasteful, or inefficient use. From data that is reported, we know that of the tens of thousands of petitions for IVC each year, at least 63 percent over the past six years did not result in an order for involuntary commitment, indicating they did not meet the criteria for forced hospitalization.
This report will explore the evolution of North Carolina’s IVC policy and its impact. Past IVC policy and case law reflect an approach once rooted in meaningful due process with the protection of individual rights as a primary concern.
Over time, shifts in policy and culture have advanced convenience over due process to the point that one psychiatrist describes IVC as “the easy button.” Rather than avoid unnecessary commitments as required under the Americans with Disabilities Act (ADA), there is an ease with which IVCs are initiated and prolonged.
As an agency that champions the rights of people with disabilities, DRNC focused on the legal status of people under custody orders in the ED. We also focused on what happens to people under IVC while they are in EDs, suffering, waiting, and getting no actual mental health treatment beyond the administration of drugs.
ED staff were candid in DRNC’s monitoring visits, sharing their frustrations and the myriad issues they face while doing their best to manage their limited capacity and provide care and treatment for people with mental health disabilities and people with medical emergencies.
Our findings include that NC’s IVC process:
- Is overused and misused (“the easy button”).
- Does not require specialized training for magistrates, the officials in NC who initiate the IVC process.
- Criminalizes and stigmatizes people by using handcuffs and shackles as well as uniformed law enforcement officers in marked vehicles to transport people under IVC.
- Dehumanizes and stigmatizes people in crisis. Instead of protecting patients, IVC laws create more trauma such that some EDs strip search people, take their clothes and belongings, and force them to wear hospital gowns. Some lie in the open on gurneys in brightly lit, chaotic EDs. Some EDs use powerful drugs, sometimes by force, and/or restraint devices to control behavior and freedom of movement.
- Allows children and adults being considered for IVC to remain in EDs for days, weeks, and even months without a legal requirement for representation or hearing.
- Causes some people, due to long, forced hospitalization, to lose jobs or housing and incur huge medical debt for care they didn’t seek or want.
- Harms people who work in the system, causing moral distress to staff who are trying to care for people stuck in their EDs.
- Harms our communities by diverting law enforcement officers away from essential tasks and making them spend thousands of hours supervising and transporting people, even sometimes waiting with patients while hospitals find beds.
- Lacks a competent data collection procedure that would enable policy makers and the public to see how many behavioral health crisis-based ED visits actually result in forced hospitalization. Without data and transparency, it is difficult for lawmakers, communities, and the populations directly impacted by the system to assess where and how processes break down.
- Removes basic rights enjoyed by others who are hospitalized, such as the immediate loss of the right to leave and the ability to possess a cell phone or other electronic device.
- Excludes and prohibits parents and legal guardians from having any voice about the treatment or hospitalization of their child.
- Infringes on Second Amendment rights and can prohibit anyone otherwise qualified for a career in law enforcement unless they endure a complex process that can cost thousands of dollars to remove the IVC from their record.
And yet, there is also good news.
NC is home to bright, innovative people. We met some of these people who are leading NC into a new landscape, one that honors people experiencing crisis, their dignity and humanity, one that understands community and connection, not coercion, as the way forward. This is already happening in pockets around NC, demonstrating how to better utilize our resources and improve outcomes. We need more.
In addition, under the leadership of Division Director Kelly Crosbie at the NC Division of Mental Health, Developmental Disabilities, and Substance Use Services, along with increased funding from the North Carolina General Assembly, the NC Department of Health and Human Services (DHHS) is launching substantial efforts focused on developing and delivering more services that will help North Carolinians get the care they need so they don’t get to a crisis situation, and if they do, offering community crisis resources to keep people out of EDs and hospital beds.
This report brings together the very real harm to children and adults thrown into NC’s IVC process and the very real successes of kids and adults who survived this system – not because of their IVC but in spite of it. DRNC is making findings and recommendations for policy, practical, and cultural change that prioritize mental health recovery, reduce forced hospitalizations, and create a mental health service landscape that is trauma-informed, effective, healing, and that minimizes fraud, waste, and abuse.
Finally, it is vital to understand that the answer to this crisis isn’t to increase the number of psychiatric hospital beds; the answer is to ensure kids and adults can get the mental health services and treatment they need, when and where they need it. Simply put, NC needs robust mental health services in our communities. We must prevent crisis from happening to begin with. We must keep people healthy, in their homes, in their communities, where they can thrive and be successful.
Isn’t that what we all want – to stay healthy, be in community, thrive, and succeed? People need healing and hope. It is no different for people with disabilities. NC must address the harm, the legal limbo, and the human and financial costs with determination and urgency.
A note on the scope of this report – IVC is used on people with mental health disabilities, substance use disorder (SUD), and intellectual or other developmental disabilities (IDD). Throughout this report we have focused on mental health. This information applies to people with SUD, IDD, and co-occurring conditions who are facing IVC as much as people with mental health disabilities.
Monitoring Emergency Departments (EDs)
The barefoot first-grader with dark hair and dark eyes was energetic. He was darting in and out of his room, grinning mischievously, playing a game with his sitter. His sitter was patient and attentive.
The boy was wearing shorts and a colorful tee shirt. His sitter, however, was wearing a security officer uniform. While the boy was playing a game, his sitter was doing her job to ensure he remained safe and secure in the hospital ED where she worked and where the little boy was confined.
DRNC staff met the boy while monitoring in the ED last year. He’d been in the ED for two weeks, awaiting psychiatric hospitalization in another facility. He’d arrived in the middle of the night in the back of a police car.
Hospital staff were doing everything they could think of to keep him happy, unrestrained, and unmedicated while they waited for a facility to agree to take him. A radiologist was using her lunch hour to read to him. The local Sheriff’s Department sent an officer with their police dog so he could go outside, get some fresh air, and pet the animal. Various staff brought him treats. Staff made sure he had a room with a window so he could see outside.
A hospital administrator spoke to us about the boy with tears welling in his eyes. There was only so much they could do.
“It is heartbreaking,” said an ED staff member.
As for the seven-year-old, he just wanted to go home.
This hospital ED is one of 10 DRNC monitored over the past year to develop a first-person understanding of how NC’s IVC commitment process works in practice. Because forced hospitalization is so restrictive, it is supposed to be an act of last resort and used only when no other alternatives have helped.
Throughout the state, no matter where, we heard story after story about children being “stuck” in EDs with no access to education, socialization with peers, real play time, the outdoors, or actual mental health treatment while they awaited psychiatric hospitalization.
“Write that down,” one hospital administrator instructed a DRNC staff member during a visit to his ED, specifically speaking to the problem of kids languishing in EDs. “It’s just the saddest thing.”
It wasn’t just kids stuck in hospitals that administrators expressed concern about, however. They shared myriad concerns with DRNC.
For context, the hospitals we monitored are in geographically diverse counties throughout NC, ranging from EDs with a dozen or fewer beds to large EDs, including two Level 1 trauma centers that provide the highest level of care to critically injured patients. The EDs were in urban and rural areas, spanning from the coast to the mountains. A few hospitals had separate psychiatric units; most did not. We monitored in local, community-owned hospitals, non-profits, and hospitals owned by large healthcare systems.
Despite their differences, common themes and experiences emerged among them.
Findings
- Many people can’t access the behavioral health services they need to keep them healthy in their communities. Left without effective care, they wind up in crisis and at an ED under a custody order.
- This system is expensive, wasteful, and abusive, relying on costly ED and inpatient psychiatric care instead of care in communities that costs far less and is more effective.
- Many people, kids and adults, who are coming through this process have trauma histories that are triggered and exacerbated by being in EDs and subjected to forced treatment. These damaging experiences make some people reluctant to seek out psychiatric care when needed.
- Kids get stuck in EDs, brought there by desperate family members or social workers from county departments of social services (DSS) who can’t find effective community services to help.
- Children and adults who have intellectual and developmental disabilities also languish in EDs awaiting beds.
- Nursing homes and assisted living facilities misuse the IVC process to “dump” people with dementia.
- Spouses and domestic partners misuse the IVC process as a means of control.
- Some magistrates issue custody orders for IVC without understanding the legal criteria and defer to people requesting the IVC, resulting in people wrongfully being taken into custody by law enforcement for an examination at an ED.
- There is no legal requirement for public attorney representation or judicial oversight while people are detained EDs.
- Hospital EDs request an IVC simply for a patient’s transportation to an admitting facility by law enforcement because there is no other way to get to inpatient treatment.
- Law enforcement agencies expend a tremendous amount of time transporting people, including small children, diverting their services from the community.
- ED staff experience stress and moral distress when facing children and adults stuck in EDs and suffering without access to appropriate mental health treatment.
We also saw starkly different approaches to care.
EDs do not specialize in mental health care or treatment but still are tasked with keeping other patients and staff safe. This can result in power struggles and the traumatizing use of forced medications and people being strapped to chairs, beds, and boards.
“We tend to lean more on chemical restraints,” than mechanical restraints, one hospital administrator told us. (“Chemical restraints” essentially means overmedication, while “mechanical restraints” refers to, for example, being tied down.)
At one small, rural hospital, two men under IVC custody orders languished in the open on medical gurneys beside a nurse’s station because there wasn’t a private room available to them. The men used their sheets to cover their heads, perhaps to shield them from the bright lights and busy activity around them, and perhaps to provide some measure of dignity. Three other behavioral health patients were in private rooms.
At another hospital, DRNC staff witnessed a man in what is known as “four-point restraints,” meaning each hand and each foot was strapped to the bed he was lying on. A staff member was assigned to remain with him while he was being restrained.
“This is almost like science fiction to me,” one hospital ED staff member reported to us. “I am watching what is happening to human beings and wondering, are we actually helping people?”
Practices that take away a person’s autonomy cause trauma and negatively impact an individual’s willingness to seek treatment in the future. They also “correlate with issues in the workplace,” said Dr. Micah Krempasky, a psychiatrist who serves as Chief Medical Officer for Mental Health and Well-Being for WakeMed Health and Hospitals.
Under Dr. Krempasky’s leadership, WakeMed is focused on utilizing trauma-informed practices. She says providing patients with care that is trauma-informed honors and values patients as well as staff – often reducing power struggles and escalation of potential violence.
Part of this training is to help medical staff understand the process of mental health diseases. “Their actions are symptoms of their disease,” she said.
Many mental health training methodologies focus on “de-escalation” techniques, teaching staff how to reduce tension in a conflict. But Dr. Krempasky flips that technique. Instead, she and her team provide “non-escalation training” to hospital staff so they can prevent conflict from occurring. “If a patient says ‘no, this isn’t a good time,’ then staff is to hear the ‘no.’ This helps empower a person who is then able to maintain dignity, respect, and control.”
WakeMed is also staffed such that an individual who comes to the ED in a behavioral health crisis will see a mental health professional within 15 minutes. Further, many law enforcement officers know to call the ED when they are on their way to WakeMed with a patient so a member of the mental health team meets them at the car upon arrival.
Dr. Krempasky acknowledges WakeMed has a benefit because it is in an attractive area to recruit nurses and doctors and they have been able to make investments in staff, and not every hospital has the same resources.
Still, DRNC met hospital staff in smaller hospitals in the western part of NC who are taking innovative actions that work for their circumstances.
NC’s IVC process begins with magistrates
The IVC process begins when a person, called a “petitioner,” goes to the local magistrate with a request (called the “petition”), to have an individual (called the “respondent”) committed to an inpatient facility for treatment for mental illness or substance use. If the magistrate reasonably believes that the facts in the petition are true and the respondent is probably mentally ill, dangerous, and in need of treatment, then the magistrate must sign an order for IVC and custody.
Under the magistrate’s custody order, law enforcement, or another designated transporter, brings the respondent to a hospital or other facility for a first examination. The first examination must happen within 24 hours of the respondent’s arrival at the facility for the examination.
Of concern, the bar for issuance of this custody order is low. NC commitment law requires the magistrate to issue the order so long as the magistrate determines the allegations are probably true, even if the petitioner did not have first-hand knowledge of the facts alleged.
If the custody order is granted, the individual loses the right to make their own decisions.
NC does not require magistrates to be lawyers, or have specialized training about the IVC process. Within six months of taking office, they are mandated to have at least 40 hours of civil and criminal training. Pursuant to law, that “basic training” is provided by the School of Government (SOG) at the University of North Carolina. According to the SOG, four hours of the civil training is focused on the IVC process, and the instructor provides the magistrates links to videos to watch in advance of the training.
After magistrates complete their basic training, NC law mandates they complete at least 12 hours of training each year, specifying seven areas in which they must complete this annual training; IVC is not one of the areas. Yet the potential harm to affected individuals is severe, including being taken into custody – loss of liberty – without legal representation until much later in the process.
If they choose, magistrates can elect to attend a two-day training focusing entirely on the IVC process. Mark Botts, associate professor of public law and government at the SOG who is widely recognized as an expert in NC’s IVC process, developed that two-day training. The course materials illustrate the complexities of the law. Botts said he occasionally presents a one-hour session on IVC topics at the magistrates’ spring or fall conference.
Botts said attendance at the annual two-day voluntary training averages about 20 magistrates per year. That represents 2.8 percent of the nearly 700 magistrate positions statewide.
Recommendations:
- Amend NC law to require specialized training in the IVC process, including the collateral costs of IVC.
- Train magistrates on the trauma that IVC causes and the benefits of NC DHHS’s crisis services information, including access to Peer Warmline, 988, peer support, and trauma-informed recovery models.
- Magistrate should inquire whether respondent has an Advance Instruction for Mental Health Treatment, also known as a Psychiatric Directive (PAD), and if there is one, that it is being followed.
- Amend NC law to make custody orders conditional on an in-person screening by a local mobile crisis team. This screening is an independent prescreen for IVC criteria and available alternatives to meet the person’s needs. Mobile crisis teams exist and will require funding for this expanded role.
- Require magistrates to inquire about efforts to avoid IVC, including calling the peer warmline, 988 or enlisting other crisis resources, prior to signing a custody order.
- Require magistrates to consider the social costs of IVC, including time out of work or school, stigma, medical costs, and trauma. If the facts, as alleged, are true, would any benefit of the commitment outweigh the likely costs?
- Require magistrates to have training in and utilize trauma-informed approaches.
“IVCs were passed out liberally”
WakeMed recognizes that IVC practices can jeopardize patient well-being. As a result, the hospital embarked on an initiative to reduce IVCs and safeguard patient rights. The initiative resulted in a 60 percent reduction of IVCs, where the vast majority of the individuals sought voluntary treatment, according to Dr. Krempasky.
Similar to the WakeMed initiative, Avery and Watauga counties also dramatically reduced their IVC rate, by 60 percent. Prior to this initiative, “IVCs were passed out liberally and there was a lack of understanding of the long-term impact,” said Stephanie Greer, president, Avery Healthcare Market over Cannon Memorial Hospital and Appalachian Behavioral Health Hospital in Linville. “Magistrates were begging for guidance.”
She said the magistrates enlisted Botts from UNC’s SOG for training help. This effort was part of a larger effort Greer initiated in 2010 to shorten the length of stay (LOS) in the EDs in Avery and Watauga hospitals, as well as reduce law enforcement hours and the use of IVC. She convened a community task force that included hospital and law enforcement officials, clerks of court, district court judges, mental health providers, managed care organizations (MCOs) and others.
Greer said the work was achieved through a cohesive “team approach with the commitment of doing the right thing for the person you serve versus the agency.” There was one rule: participation on the task force was strictly limited to individuals who had decision-making authority. At the end of each meeting, an “action plan” was created and people held each other accountable for their tasks. She said some of the meetings were “uncomfortable,” but they pressed on, unified in their desire to improve the systems and the well-being of the people they serve.
At one of the meetings, a district court judge suggested that mental health assessments happen before a magistrate signs a custody order. The task force’s work had already resulted in the creation of a “crisis unit,” comprised of clinicians at Watauga General Hospital and Cannon Hospital. So this crisis unit began conducting mental health assessments for children and adults presenting in their EDs, while community mobile crisis units were called to conduct assessments for petitions originating at local magistrate’s offices.
The result according to Greer: magistrates now issue custody orders only 40 percent of the time.
This community task force was also successful in its efforts to reduce LOS in the EDs. In 2012-2013, Greer said the average LOS was 27 hours. They were able to reduce that time to six hours, saving hospital ED resources, law enforcement resources, and most importantly, reducing the toll on the people forced into the process.
“One size does not fit all,” Greer said of the work their community task force accomplished. “You have to give autonomy to the communities that are engaged. The ‘what’ you have to accomplish is not negotiable but the ‘how’ to get there is. Solution approaches have to be different for different communities.”
Every hospital ED we visited was focused on finding ways to shorten the length of time people spend in their ED, recognizing that hospital EDs are not therapeutic environments for people experiencing a mental health crisis. Using EDs in this way also taxes the provision of medical care for people who require emergency treatment.
And there is another important liberty issue: While someone remains in an ED under a custody order for IVC, there is no judicial oversight to determine whether the magistrate’s custody order is appropriate or even legal without hiring a private attorney.
For example, Ben[2] was involuntarily hospitalized based on a blank petition a magistrate approved while the young man was in an ED. The petition is required to state reasons for the initiation of the IVC process, but this one had no facts alleged. Even though the “Facts” section was blank, the magistrate signed the custody order.
A day later, the hospital ED identified an available bed in a psychiatric hospital. Law enforcement then shackled Ben’s hands and feet and transported him in a law enforcement van to a hospital three hours away. Once admitted to the psychiatric hospital, known by NC IVC law as the “24-hour facility,” he was assigned a lawyer known as “special counsel” as required by law. The lawyer immediately spotted the issue and submitted a motion to a judge, who dismissed the IVC. Despite the judge’s order, the hospital illegally held Ben for five more days.
Importantly, the appointment of special counsel and a judge’s review of the custody order only happen after someone is transported to the 24-hour facility. The appointment of the special counsel is the first time NC law affords due process to the individual. At the judicial review hearing, the judge determines, finally, whether the person meets the legal criteria for civil commitment. If so, the IVC commitment order is issued.
As later explored more in depth, a commitment order can remain in a person’s record permanently, damaging future career prospects, rights and privileges. Based on DRNC’s review, the majority of petitions do not result in an IVC. Yet lasting harm may be done to people at the center of the petition and custody order.
Sam’s story
Sam4 is 34 and has a 10-year history of saving lives as an emergency medical technician (EMT) and a volunteer firefighter. He lives in western NC, enjoys spending time with his girlfriend, and also works at her parents’ business to make ends meet.
Life wasn’t always so sunny for Sam. As a teen, he dealt with an abusive father, and his mother struggled with mental health challenges. As a result, Sam also struggled and at 15 he was involuntarily committed. Following that hospitalization, he thought he’d closed the book on that painful chapter of his life.
He went on to serve in the National Guard as a military police officer, as an EMT, and as a volunteer firefighter. Recently, he was recruited by a local law enforcement agency to become a law enforcement officer. Sam eagerly signed up for training at NC’s training academy.
But while he was going through that training, the law enforcement agency that recruited him alerted him that he did not pass the firearms background check. His name came up on the National Instant Criminal Background Check System (NICS). A letter from the Federal Bureau of Investigation (FBI) subsequently notified him he is designated on the NICS as “a person who has been adjudicated as a mental defective or who has been committed to a mental institution.” Federal laws do not allow people who have been committed under IVC to use, own, or possess guns.
Sam was floored. He wasn’t even aware he’d been involuntarily committed when he was hospitalized at 15.
“Having to jump through so many hoops just to get your own record is ridiculous,” he said. “I’m worried that if I can’t get this taken care of, then I might not be able to pursue a career that I want to. It’s scary that you might not even know that you have been IVC’ed until it’s too late, and how it can slip through some cracks but not others. Like it not showing up when I joined the military and obtained a secret security clearance but showing up when I applied for a personal firearm while in Basic Law Enforcement Training. Feeling like you are being taken advantage of when you try to obtain a lawyer to get an expungement and them quoting you $10,000 just to look into the issue. It feels like the system is against you in every way if you don’t have the money or resources to fight it.”
His mother feels guilt and shock.
“He was a screwed-up kid in a bad set of circumstances,” said his mother. “He was able to rise above it all and become an amazing adult. He will make an outstanding officer. He has been very responsible. He has managed his issues. He deserves a normal life. Not to have his dreams crushed at 34 for something that happened when he was 15 that wasn’t even criminal.”
Sam may be able to have his IVC expunged from court records. Expunging his IVC record will give him a second chance to pursue a career in law enforcement. However, it is involved and can be expensive. One lawyer was willing to help Sam for a $10,000 fee, which is a hefty sum many people cannot afford.
Fortunately, DRNC is able to help Sam with this process.
Even though the US Constitution protects people’s right to keep and bear arms, once a person has been involuntarily committed and their data is included in NICS, they cannot legally own or possess a firearm. The person may be disqualified from military service or law enforcement professions. They also cannot engage in hunting, recreational shooting, gun collection or keep a gun for their personal safety. This is the case even in instances where the IVC statutes were misused, such as a person who was involuntarily committed because a spouse took out a petition to gain the upper hand in a divorce or custody lawsuit.
While federal law does not require states to report identities to NICS, NC lawmakers mandated that information about people with IVC commitments be reported to NICS.
Access to NICS is limited to law enforcement agencies and firearms dealers.
While an IVC report to NICS is an infringement on Second Amendment rights, an IVC also has the potential to affect other rights and privileges. Any party can challenge a potential juror on the ground of “mental infirmity.” The United States Supreme Court has ruled that a judge can determine whether a person can represent themselves in legal proceedings based on mental capacity.[11] Additionally, mental incapacity is a ground for terminating parental rights. IVCs involving substance use may result in driver license revocation.
Due process denied in hospital EDs
“The laws weren’t written with the knowledge it may take days, weeks or months to get a bed. I don’t think anyone wants that,” said Dr. Krempasky, referencing the fact that people can remain in EDs without representation or judicial oversight.
Under NC law, the custody order that requires the person be examined at the ED lasts for seven days. If not renewed, the person must be discharged from the hospital. If the order is renewed, “you can have successive custody orders, each one for a seven-day period,” said Botts, the IVC law expert at UNC’s SOG.
“Consequently, there are cases where the respondent is held for weeks without legal representation or a hearing. Successive custody orders create a loophole in the requirement to provide the respondent legal representation and a hearing within 10 days of being taken into custody, because the statutory law does not afford that due process until and unless the respondent is transported out of the ED to a psychiatric inpatient facility.”
“That is a big loophole,” Botts said.
This can go on indefinitely.
“So, the patient is not free to leave, the patient is under a custody order, they are being held involuntarily, but they are not being provided treatment, which is ostensibly the very purpose for which they are being held involuntarily,” Botts said. “All of this happens before they even get to a psychiatric facility, and unless and until they get to a psychiatric facility, they are not going to be provided counsel. There is very little due process but there is full deprivation of liberty.”
“This is particularly problematic,” Botts said.
Data about these successive seven-day petitions is not kept, so there is no way to know how often this is happening, or where.
Botts stressed that the loss of parental rights is another troubling problem in EDs. Parents or legal guardians of minors take their child to an ED seeking voluntary care, but instead the ED petitions the child for IVC and the parents are “pushed to the side.”
“Upon invoking the IVC process, some hospital EDs stop consulting and sharing information with the parents, even though the parents retain a statutory right of access to their child’s health care information,” Botts said. “Parents will be at the ED one day and return the next day to visit their child, only to find their child is no longer there, having been transported several counties away to a psychiatric inpatient facility. Sometimes the very family members who play an essential therapeutic role in the child’s life, who have the best information about the child’s mental health and who are essential to health care decision making, are kept in the dark. Once the IVC process is invoked, it is as though the parent is not there. And the parent has no choice where their child is sent.”
That was the experience of Megan and Dan, Durham parents of then 11-year-old “Marie,” whose traumatizing experiences with the IVC process were chronicled by North Carolina Health News in 2022. “It was clear to me we didn’t have a say in anything and that’s very upsetting,” Dan recently recalled to DRNC. “That’s one of the hardest things – the helplessness. It was very hard to learn we were not in control of what was going to happen to her.”
Megan agreed. “It took a while for that to sink in.”
While “not perfect,” Marie was safe during her three nights at the ED at Duke Hospital in Durham, they said, but they were completely unprepared for what would happen to Marie once she left there, taken away by uniformed police officers and transported to a hospital three hours away whose online reviews frightened them.
Dan and Megan desperately wanted to take Marie home and find care from there. “We will sign a waiver releasing liability,” Dan, a lawyer, said he told the ED staff. “We will watch her 24/7. I know she needs a higher level of care, I’m not denying that. You just can’t take the control away from us,” he remembers pleading with staff.
But once the IVC petition process was initiated, there was nothing Megan or Dan could do until Marie’s rights under NC statutory protections kicked in, and that would not be for several more days.
“I can categorically say that was the worst week of my life,” Dan said. Marie and Megan immediately concurred. “Me too, me too,” they said.
NC law has an explicit preference for voluntary over involuntary treatment. That is not the reality.
Recommendations:
- Amend NC law to require that IVC petitions of adults under guardianship and children include information about the legal guardian’s and/or parents’ involvement in seeking and planning care and why voluntary treatment could not meet the respondent’s needs.
- Amend NC law to eliminate successive petitions.
- Amend NC law to appoint special counsel or contracted appointed counsel at the time magistrate issues the custody order so respondents can have timely representation. This new provision must come with funding to pay for the additional staffing that will be required.
- Supportive parents, legal guardians, and caregivers should not be excluded from communications and medical decisions. Require ED staff assigned to care for minors and adults under custody orders have training in and utilize trauma-informed approaches.
- Promote the execution of Advance Instruction for Mental Health Treatment, also known as Psychiatric Advance Directives (PADs) and educate stakeholders, including ED staff, about the purpose and meaning of PADs.
Misuse and overuse of the IVC process
We spoke to numerous ED staff and administrators who reported that some people, businesses, and agencies use the IVC process inappropriately. This misuses precious resources and illegally deprives people of their liberty. While the civil commitment process is not a criminal process, it has all the hallmarks of a criminal process: people are locked up and are often transported by law enforcement in shackles.
“In my opinion, the IVC process is broken,” said Rusty Miles, director of the ED at Carteret Health Care in Morehead City, located on the coast. Miles’s reflection was not an outlier; we had several hospital administrators lament the misuse and overuse of the IVC process. “It should only be used if the person is a safety risk for harm to self or others,” Miles said.
He says he’s seen people use IVC “to make a statement to their partner that ‘I can do this to you,’” or for people who have overused alcohol, for example. “You can’t IVC because of bad decisions,” he said.
Nearly universally, frustrated administrators reported that some nursing homes or assisted living facilities routinely take out IVC papers and “dump” patients with dementia at their ED. These facilities know the hospitals will be forced to take them under a federal law that prohibits hospital EDs from turning away people who present for help.
“That’s a medical issue,” said one ED nurse. “There’s no reason for a dementia patient to be under IVC because it’s a medical condition, not a psychiatric condition. My first question is, what’s the treatment plan? How is this going to get better? This is a huge issue.”
Children are also “dumped” in EDs. Sometimes they are taken there by frustrated family members or caregivers who can’t get services that are appropriate and helpful to the child. The IVC process is used as a legal lever for finding care for the child.
But the more frequent complaints regarding kids centered on staff with local departments of social services (DSS) who drop off kids at EDs. These are children and youth who have been removed from their homes due to abuse or neglect allegations. When the local DSS agency is unable to find placement with a foster family, they must find some place for the children to live.
One hospital administrator said they have had DSS agencies from the western part of the state drop foster kids at his ED, several hours away. He shared this information last summer, before Tropical Storm Helene hit Western NC; Helene was not the reason. Staff with an ED in the central part of the state similarly reported DSS agencies from all over the state drop foster children at their ED.
These are the children who often spend the longest time in the hospital EDs because they have complex mental health needs, and it is difficult to find a psychiatric facility that can provide the right treatment for their individual needs. These children have already experienced the traumas of neglect or abuse, removal from their homes, schools, and communities, and find themselves in an ED, confined to a tiny room, surrounded by ED trauma, 24/7. They are isolated from family and friends in a strange place and maybe in an unfamiliar town.
“The DSS interplay with the system is problematic,” said an attorney who represents children who are IVC’d. “I can appreciate it is hard for the DSS agencies, but it is not a receptacle for kids. I would be interested to see what can be done about DSS using hospitals as dumping grounds.”
One NC hospital administrator turned to the law. His hospital communicated with DSS agencies indicating a willingness to sue for room and board. He told DRNC that each time they did that, DSS staff picked up their kids within days of the communication.
“People are manipulating the system out of desperation,” said Avery Healthcare Market’s Greer. “The majority of the time [people are dropped at EDs] it’s because people are desperate and they don’t have a solution.”
A year ago, NC DHHS announced an initiative that would provide nearly $8 million over two years to DSS agencies across the state to help them identify emergency placement settings for children who are in DSS custody, but the issue remains.
“It’s a real challenge,” said Miles, the ED manager at Carteret Health Care. “I’m going to be real honest: These kids don’t get the services they need, they miss school, socialization, and outside play. We do the best we can but it’s a real disservice to keep these kids here. But we do all we can to keep them safe.”
People should not have to pay with their liberty for the failures of the system. The negative impacts can be life-long.
Recommendations:
- Community-based care must be expanded and funded with urgency to prevent overuse and misuse of EDs.
- Explore shifting costs to petitioners for frivolous or repeated IVC-related expenses. If health care providers routinely choose to pursue IVC, they must bear some risk for the financial cost of that forced treatment. This would be especially helpful in the case of Adult Care Homes and Skilled Nursing Facilities that use IVC petitions to move residents off their caseloads and into more expensive hospital settings, circumventing discharge planning requirements. Shifting costs would require extensive study and planning but could dramatically reduce the number of IVC petitions filed simply because they were the path of least resistance.
Transportation concerns
Ben[3] vividly recalls his transport from the hospital ED near his home in the south-central part of NC to a psychiatric hospital three hours away. No one told the then 21-year-old where he was going or how long the trip would take.
Even worse, a uniformed law enforcement officer shackled Ben’s hands and feet and put him into the back of a marked law enforcement transfer van with no windows. “I don’t think you should be transported in shackles. I don’t think that’s okay,” he said. “Basically, I was treated like a criminal who got dropped off at a hospital for medical treatment on the way to go to prison.”
Ben’s experience is like many others’. And there is widespread support for improving the situation.
The law allows for the use of shackles, called “restraints,” but not as the default, as is often the case in NC. “Any use of restraints shall be as reasonably determined by the officer to be necessary under the circumstances for the safety of the respondent, the law enforcement officer, and other persons,” according to the law. Children are also subjected to transport by law enforcement, an especially traumatizing event given the vulnerability of their age and compromised mental awareness during a crisis. NC law specifically notes special considerations in the use of shackles for children under the age of 10, though still allows officers to shackle them.
It’s unclear why Ben was shackled for his drive; he was alone in the back of the van, physically and structurally separated from the sheriff’s deputy.

Ben knew it didn’t have to work that way. Two years earlier during a mental health crisis he’d been assessed for IVC at a different hospital ED and that hospital arranged private transport by a woman in an unmarked vehicle. He was also told where they were going. “I was transported in a totally different way, so it’s not like they can say we can’t do it differently, because they did it that time.”
Ben’s account reflects the inconsistent experiences people under IVC may have, simply based on where they are in the state when the IVC process initiates. Amid the rising numbers of IVCs across the state spanning more than a decade (as discussed in depth below), the state’s increasing population, and the lack of appropriate and accessible community mental health services, law enforcement became the default for IVC transportation.
And while NC law allows for a mental health provider, family member, or friend to transport an individual under certain circumstances “if they so request,“ that information is not widely shared, and requires authorization by a clerk of court, a magistrate, or a district court judge.
Megan and Dan, parents of Marie, would have leapt at that provision had they known it existed when two uniformed police officers transported then 11-year-old Marie in a marked police car from Duke Hospital in Durham to a hospital three hours away.
She would have been the ideal candidate for that three-hour ride. “She was zero threat,” her dad told DRNC recently. “Everyone acknowledged she was no threat.”
Worse, the transporters intended to handcuff Marie. Duke doctors and staff tried to convince them not to put the cuffs on her; Megan said some of them were in tears. Had it not been for an “angel” family friend and staff member at the hospital who unexpectedly showed up at the scene and successfully dissuaded the officers from using the restraints, Marie would have been handcuffed.
The experience was traumatizing to the family. “The police officers did not introduce themselves, they literally plopped her into the back of the car and zoomed off,” Megan said. “They were not nice; they were not comforting.”
The hospital let Marie take the blanket she’d been given when she arrived at Duke’s ED three days earlier, and she used that to try to find some measure of comfort on the hard back seat, separated from the officers in the front seat by a partition. Finally, she covered her head with the blanket and tried to sleep.
Marie said the officers spoke to her only once. “They spilled something, and they said, ‘We’re getting out of the car now.’” That was all they said.
They instructed Dan not to follow them closely. He did not understand why, but he complied. That meant he didn’t get to Brynn Marr when Marie did. “I got dropped off, and I was like, ‘Where’s Dad?’” Marie said.
Like the officers who transported Marie and Ben, law enforcement officers across NC routinely spend hours transporting people to hospital beds, often times out of their counties and sometimes across the state. for transporting a person to a hospital for a first examination in the IVC process, as well as transporting them to the facility where they undergo forced treatment. Once the person is discharged from the treatment facility, the same law enforcement agency must travel to pick up the person from the hospital to return them to their home county.
![]()
View text version of law enforcement transport graphic
Requiring law enforcement to transport children and adults is a misuse of their resources and can be dangerous for people in a behavioral health crisis. Law enforcement transport for IVC squanders community resources, elevates tension, and increases risk of harm as well as lasting stigmatization.
By law, transportation is left to local authorities to design and can include alternatives to using law enforcement, such as contracted transportation as occurred in Ben’s earlier hospitalization. But most counties still rely on law enforcement as their method of transport.
When law enforcement transport is used, the law requires that “to the extent feasible,” every effort “shall” be made for the transporting officer to be the same gender as the person being transported, to wear plain clothes and drive an unmarked vehicle. If the officer is not the same gender as the person being transported, then the law enforcement officer can allow a family member of the person to ride with them. DRNC is not aware of any situation where this was allowed.
The limited available alternatives to law enforcement transport and a mistaken belief by some EDs that law enforcement must transport someone to a psychiatric hospital are key drivers for the misuse of the IVC process and to the continuing overuse of law enforcement for transportation in the IVC process.
“It’s the easy button,” said WakeMed’s Dr. Krempasky. To prevent unnecessary law enforcement transport, WakeMed chose to foot the bill for transportation, whether via IVC or for voluntary commitments.
Avery Healthcare Market’s Stephanie Greer said 15 years ago, local officials in Avery and Watauga counties decided to address the amount of hours law enforcement officers were spending in mental health processes, as well as the overuse of IVC and diversion from EDs.
The results from their work are astounding. In 2010, for example, Watauga County law enforcement spent an average of 2,800 hours per month for behavioral health processes. Three years later, that average was reduced to 419 hours, and by 2015, the average plummeted to 120 hours per month. Their work shows that when communities come together to solve an issue, they can design systems that work for them.
Physicians, hospital staff, parents, and the children and adults who have experienced law enforcement transport are not the only people concerned about the traumatic and inefficient transportation process. The NC Sheriff’s Association has advocated for local mental health professionals to take on the responsibility for transporting people during the IVC process. In its “Report on Law Enforcement Professionalism,” updated in 2022, the association seeks changes in state law to shift transport duties from law enforcement officers to mental health providers. That same year, the NC Sheriff’s Association published information and guidance for law enforcement officers who are involved in the process. Notably, law enforcement officers themselves recognize they are not the best option for IVC transport.
Transylvania County Sheriff Chuck Owenby is empathetic to people who need mental health services and wants to see more services provided in the community. He wants people to get the help they need. He also says his small staff’s IVC transportation efforts dilute their traditional law enforcement coverage in the county. “The biggest burden for me is it’s a strain on the office,” Owenby said to a Transylvania Times reporter recently for an article entitled, “Lack of mental health services burdens Sheriff’s Office.” Like many people entrenched in the IVC process, he is eager to find solutions. “Mental health-wise, I’m willing to listen to anyone if it gets people the help they need.”
A recent national study from Duke University’s Wilson Center for Science and Justice explores alternatives to law enforcement transport for people in behavioral health crisis and provides a compelling overview of practices across the country and in NC. “Not only does law enforcement involvement blur the lines between treatment and criminalization of mental illness, but law enforcement officers also widely report that they do not feel well-equipped to handle mental health crises,” report co-author Dr. Marvin Swartz, Professor of Psychiatry and Behavioral Sciences at Duke University and Wilson Center Behavioral Health Core Faculty Member said in a news release when the report was issued last fall.
Dr. Swartz said a goal of the report is to help communities develop new transport policies “that minimize interaction with law enforcement to benefit both people experiencing mental health crises as well as redirect law enforcement time and resources to issues better suited to police involvement.”
According to the Wilson Center study, “People with serious mental illness are over eleven times more likely to experience law enforcement use-of-force and over ten times more likely to be injured in law enforcement interactions compared to other individuals,” the study states. “Racial biases and prejudices further exacerbate these outcomes, as Black people are already disproportionately more likely than white people to experience force at the hands of law enforcement.”
NC DHHS is now stepping up to fund pilot projects that explore alternatives to police transport, using a $20 million boost from the NC General Assembly. “It’s not a good setup for individuals who need crisis care. Certainly, not a good setup for the law enforcement officers either,” said Kelly Crosbie, director of DHHS’s Division of Mental Health, Developmental Disabilities, and Substance Use Services in December when the department announced the $20 million program. “When someone raises their hand and says I need help, that’s a miracle. It is. And it is our job to respond to that in a compassionate, therapeutic, and actually helpful way.”
To develop one or more pilots, DHHS created a competitive Request for Proposals for organizations that will provide Non-Law Enforcement Transportation (NLET) in two different geographic regions of the state. The department called NLET “a promising practice of providing trauma-informed transportation for people in mental health crisis who need to be transported from emergency rooms to residential treatment.” As of the writing of this report, the RFP process has closed.
Recommendations:
- Amend NC law and Medicaid policy to require public and private insurance companies, MCOs, and Medicaid to fund and enter transport agreements with appropriate non-law enforcement providers to transport people to and from available inpatient mental health facilities in a trauma-informed manner.
- In the meantime, where law enforcement agencies must be used, NC law must be amended to remove discretion about the use of shackles, uniforms, genders of transporting officers, and marked cars. If a law enforcement officer believes the use of restraint, including handcuffs or shackles, is required, they must seek prior authorization from a commanding officer and file a written report detailing the reasons restraint was necessary and the outcome.
- Require facility providers to notify the respondent and their parents, legal guardians, and/or family members, about the option to transport the child or adult themselves. This should be done verbally and in writing.
- Require all transporters be trained in and utilize trauma-informed approaches.
Getting first examinations and length of stay in EDs
When someone arrives in an ED for examination under a custody order, ED staff have 24 hours to ensure the commitment examination occurs. In the meantime, people are typically stripped of all of their clothing and possessions, searched, and provided hospital scrubs, or worse, a paper gown.
ED staff then conduct a medical assessment that can include blood labs and a physical exam to determine whether there is a medical issue that must be addressed.
Commitment examination procedures vary widely. Some hospitals have in-house staff who are trained and certified to conduct these specialized examinations. Smaller hospitals generally contract with outside providers to provide these services, often via telehealth.
To help ensure mental health professionals are available to conduct these examinations within 24 hours in all areas of the state, in 2018, the NC General Assembly expanded the type of professionals eligible to perform this function. For years, only physicians (medical as well as psychiatrists) or licensed psychologists with two years of clinical experience could conduct these exams. The revised law now allows a broader range of licensed professionals to perform the assessments, and they must be certified to participate in the process.
The length of stay (LOS) in hospital EDs is something hospitals closely monitor. Patient “boarding,” in particular, is an issue that hospitals focus on because it adversely affects the care and treatment of patients as well as hospital staff. The North Carolina College of Emergency Physicians (NCCED) provides talking points to its members to assist them in speaking with NC legislators about the effects of ED boarding.
According to the NCCED, prolonged boarding contributes to negative health outcomes, including avoidable deaths, as well as staffing shortages and staff burnout. They cite one NC health system as saying the average LOS for behavioral health patients was 45 hours, or nearly two days. Another hospital system said their average LOS for behavioral health patients was 40.5 hours.
The NC Institute of Medicine’s recent report on the future of NC’s nursing workforce confirms the harm to health care environments when treatment delays occur. Long LOSs can contribute to an adversarial and tense environment in EDs, negatively impacting patients, health care professionals, and the community, according to the report.
Some hospitals use telehealth psychiatry for their assessments. For example, Carteret’s ED uses a telehealth program based in Greenville at East Carolina University, the North Carolina Statewide Telepsychiatry Program (NC-STeP). It was created in 2013 after the North Carolina General Assembly (NCGA) directed the Office of Rural Health within the DHHS to oversee a statewide telepsychiatry initiative, “so that an individual presenting at a hospital emergency department with an acute behavioral health crisis will receive a timely specialized psychiatric assessment via video conferencing technology.”
The NC-STeP program served 23 hospital EDs in 2024. In 2024, the average length of stay (LOS) in EDs for people seen by the program was 65.4 hours. That was down from its high of 77.7 hours in 2022. The other years generally trended lower, with the lowest being 37.4 hours in 2014.
NC-STeP’s assessments reduced the number of people who were facing IVC petitions, indicating the custody orders and detainment were not necessary because the person did not meet the criteria for IVC. Of the 3,206 people who were assessed for involuntary commitment last year, the NC-STeP assessments “turned over” 31.3 percent, which is the lowest percentage in nine years. It has turned over as many as 44 percent of IVC petitions (2018) and as few as 23 percent (2014, the first full year of its work). The patients whose custody orders were turned over were discharged from the hospital or converted for voluntary treatment. The program maintains detailed data and provides quarterly reports on its website.
For people who are discharged from the ED to the community, connection to resources is critical to successful reintegration and safety. Understanding this, in February 2025, DHHS’ Division of Public Health sent a memorandum to the state’s ED staff and allied health providers, alerting them to two alarming statistics: nearly 70 percent of people discharged from EDs following a suicide attempt don’t begin mental health treatment in the community, and for those who are actually hospitalized, their suicide rate is 200 times higher than the general population upon their return to the community. The memo was particularly geared for ED staff to provide “clear, evidence-based recommendations specifically for care transitions.”
Staggering numbers of petitions, then very little data
Of the tens of thousands of petitions for IVC each year, at least 63 percent over the past six years did not result in an order for IVC, indicating they did not meet the criteria for forced hospitalization.
And that is based on low and incomplete data.
It is impossible to fully evaluate NC’s IVC process because very little data is collected. Each of NC’s 100 county clerks of court were required to provide to the NC Administrative Office of the Courts (AOC) reports reflecting the number of petitions filed in the county by month, but some counties failed to report for some months.
The AOC says these reports, called Special Proceedings Confidential (SPC), contain more than petitions initiating the IVC process. Multiple sources estimated to DRNC that IVC petitions constitute more than 99 percent of the cases reported each month.
Over the last six years, from 2019 through 2024, county clerks of court reported on average 95,191 SPCs each year; unfortunately, these data are incomplete because some counties did not report data every month of every year, meaning the actual numbers are even higher.
It is critical to collect and analyze accurate data so policy makers can determine which adjustments to law or policy should be made to prevent the wrongful, wasteful, or inefficient use of the IVC process. “What’s not measured cannot be managed,” said Bob Ward, a retired Mecklenburg County public defender who represented people facing IVC and remains a strong mental health advocate.
While he was still practicing law as a public defender, Ward took on a project, along with others in Mecklenburg County, to track the numbers of IVC petitions statewide. NC Health News chronicled those efforts in 2020, and updated them in 2022.
DRNC reviewed and updated the numbers in those reports in preparation for this project.
This data reflects the numbers of petitions for IVC. People named in those petitions are taken to facilities, often an ED but sometimes another facility more specialized for behavioral health needs, for a first evaluation.
If the first evaluation determines the person meets criteria for IVC there is a second evaluation.
The NCGA gets data on these second evaluations included in reports NC DHHS provides annually to the Joint Legislative Oversight Committee on Health and Human Services (JLOC) pursuant to state law that requires hospitals to report certain data to DHHS. The reports list the number of individuals who were admitted to 24-hour facilities for a second assessment. The reports for the JLOC began on Oct. 1, 2019.
The legislature exempted the three state-operated psychiatric hospitals from this reporting even though those facilities also receive people under a custody order for IVC. In addition, some facilities reported incomplete data, and a few facilities failed to report any data.
This means the actual numbers are higher than provided to DHHS and the JLOC. The lack of required reporting prevents the public and policy makers from being able to fully examine and resolve the flaws in our state’s IVC policy.
The JLOC report numbers from the same six-year period (2019-2024) reflect an average of 35,410 people under IVC custody orders who were deemed to require treatment at a 24-hour facility, far fewer than 95,191, the number of petitions initially sought. That means in those six years, compared to the SPC data, only 37 percent of petitions for IVC, plus whatever unreported number went to state-operated hospitals, were transferred for involuntary hospitalization. That means an astonishing 63 percent did not meet the criteria for IVC by the first examination.
Overall, these reports clearly demonstrate an IVC system that is overused and misused.
Four years ago, the NCGA amended the reporting law to include more detailed data including: the method of transportation to the 24-hour facility (Law Enforcement, EMS, Mobile Crisis Team, Provider, Walk-in/from ED, Contract Transportation, Medical Unit, or Other) as well as the number of people moved from involuntary to voluntary status between arrival at the 24-hour facility and completion of the 24-hour exam.
For the past three years, that information has been reported to the JLOC but it is not summarized or interpreted, meaning a determined legislator would have to sift through data, facility by facility and line by line to see patterns or draw conclusions that would inform legislative or policy intervention. The most recent report, covering July 1, 2023 through June 30, 2024, is 132 pages long.
DRNC requested and received the raw data from DHHS and based on that data, determined that for State Fiscal Year (SFY) 2024, an additional 3,678 IVC admissions were moved from involuntary to voluntary admissions before the required 24-hour exam was completed. That represents just over 10 percent of the reported 35,941 admissions to 24-hour facilities.
Given what we know about the inappropriate use of IVC solely for transportation purposes this raises the specter that some of these 3,678 people may have been forced through the IVC process solely to access transportation for treatment.
SFY 2022-2024 data detail re voluntary admissions after transport to second evaluation facility:
| SFY – 2022 | SFY – 2023 | SFY – 2024 | |
|---|---|---|---|
| Switched to Voluntary After Law Enforcement Transport |
2,263 | 2,352 | 1,946 |
| Switched to Voluntary After EMS Transport |
230 | 101 | 58 |
| Switched to Voluntary After Mobile Crisis Transport |
4 | 3 | 3 |
| Switched to Voluntary After Provider Transport |
29 | 42 | 21 |
| Switched to Voluntary After Walk-In or From ED |
1,227 | 861 | 798 |
| Switched to Voluntary After Contracted Transportation |
509 | 786 | 756 |
| Switched to Voluntary After Arrival from Medical Unit |
10 | 32 | 38 |
| Switched to Voluntary After Unknown Transport |
21 | 92 | 58 |
| Total | 4,293 | 4,269 | 3,678 |
An examination of the data related to transportation methods reveals that in SFY 2024, law enforcement transported more than 68 percent of individuals under petition for IVC. Just seven percent were transported by private agencies contracted to transport. Eighteen percent involved ED walk-ins or transfer to the hospital’s psychiatric unit from its ED. The remaining six percent, in descending order, were transported by emergency medical services, “unknown,” arrived at the psychiatric unit from a medical unit, were transported by a community provider, or by mobile crisis.
SFY 2022-2024 data detail re transportation to second evaluation:
| SFY – 2022 | SFY – 2023 | SFY – 2024 | |
|---|---|---|---|
| Transport by Law Enforcement | 28,251 | 26,382 | 24,514 |
| Transport by Emergency Medical Services |
2,218 | 1,761 | 1,114 |
| Transport by Mobile Crisis | 42 | 25 | 13 |
| Transport by Provider | 247 | 305 | 150 |
| Arrival by Walk-In or From ED | 6,937 | 7,402 | 6,537 |
| Transport by Contracted Transportation |
2,218 | 2,822 | 2,687 |
| Arrival from Medical Unit | 117 | 474 | 343 |
| Unknown Transport Method | 726 | 536 | 589 |
| Total | 40,756 | 39,707 | 35,947 |
The NCGA is asking important questions in seeking the required data.
Recommendations:
- To more fully understand the issues, the NCGA must require additional reporting and interpretation of data, including:
- Category of the petitioner, i.e., law enforcement, family member, domestic partner, clinician, other, for each petition sought.
- Race, age, ethnicity, and gender for each respondent.
- Outcome of each petition, dismissal or custody order granted.
- Transport method to the ED or other site of first evaluation for people under a custody order for IVC.
- Number of people discharged from an ED after a custody order because they didn’t meet the legal criteria for commitment following the first evaluation.
- Length of ED stay for people awaiting a bed in a 24-hour facility.
- Number of successive 7-day petitions per hospital as well as per respondent.
- Number of people transported to 24-hour facilities, specified by facility of origin.
- Number of people transported to 24-hour facilities from EDs.
- Number of people discharged from 24-hour facilities prior to the 10-day IVC commitment hearing, broken out by day of stay, i.e. discharged on Day 2, or Discharged on Day 9.
- Number of people discharged from 24-hour facilities at the 10-day hearing.
- Lengths of stay (LOS) for children and adults in EDs under IVC proceedings.
- Amend NC statutes to require DHHS and AOC to collaborate and provide streamlined reporting.
- Make data readily available to policy makers and the public on an electronic dashboard.
- It is imperative that uniform data is collected consistently and published in a form that is useful and accessible to the public and policy makers.
Florida as a model for data reporting
The state of Florida is recognized as a leader for its data dashboard, which provides detailed and transparent information in a way that enables people to examine how their IVC system, called the “Baker Act,” is utilized.
Housed under Florida’s Department of Children and Families, Substance Use and Mental Health Division, the dashboard allows users to filter demographics of involuntarily committed individuals, exams, and factors surrounding initiation of exams. The dashboard provides specific counts of IVCs per facility, numbers of repeat examinations, and numbers of people with more than one IVC over a requested date range. Locations of IVCs, types and initiators of IVCs, numbers of distinct individuals examined, as well as the number of high utilizers can all be determined over a specific date range, by region and by facility.
Users can filter information by demographics including race, age, ethnicity and gender. The information is entered by facilities and displays the last date posted on the site. Data reporting and its publication to the website are required by law to assess needs and target resources in an effort to facilitate a “comprehensive and cohesive system of coordinated care for behavioral health treatment.”
Florida’s data dashboard is an example of a system that can be used as a foundation for NC policy makers to consider in developing its own dashboard. Data is critical to identify problem areas that need solutions. Until NC has a means of assessing how the IVC process plays out, people and systems will continue to experience harm needlessly.
“I didn’t get treatment, I just got locked up for six days”
As noted above, research indicates that in the month following release from inpatient psychiatric hospitalization, people who were hospitalized have a suicide rate that is 200 times higher than the general population, according to the National Action Alliance for Suicide Prevention.
People and families with whom DRNC spoke described troubling experiences that are lasting and forever shape how they view and approach NC’s behavioral health system. All described wrenching harm. All described a deep distrust of the system that has made them rethink how, and whether, they will seek help in the future.
In addition, as our state’s P&A, DRNC staff regularly monitor inpatient psychiatric settings and speak with patients who report allegations of abuse and neglect. DHHS’s Division of Health Service Regulation is charged with investigating such allegations and has substantiated numerous claims of abuse and neglect. However, those findings are not available on their website and are not easily accessed by the public.
“It’s the treatment that’s harming people, not the diagnosis,” said Cherene Caraco, founder and CEO of Promise Resource Network (PRN), a peer-led, recovery-focused organization based in Charlotte. Caraco also serves as chair of DRNC’s PAIMI Advisory Council.
Tracy Boggiano agrees. “I didn’t get treatment, I just got locked up for six days. If anything, I came out worse than when I went in,” she said.
Tracy went to a crisis facility seeking help with medications for her mental health disabilities because a new assistant to her long-standing psychiatrist would not put Tracy in touch with her psychiatrist. Though she sought voluntary treatment, she wound up being petitioned for forced hospitalization and transported there by uniformed law enforcement.
The environment she described was chaotic. Patients were not allowed to remain in their rooms during the day. There were fights and yelling. She still remembers the jarring sound of doors slamming hard.
She was not provided any medical treatment or examination for an injury to her foot that caused pain and swelling.
The psychiatrist assigned to Tracy in the facility stripped her of most of her medications, including medication that helps her sleep and medication that eases anxiety.
“I was shaking the last two days,” she said.
Once home and back in touch with her psychiatrist, the two worked together to develop a plan to help keep Tracy safe and in the community. Her psychiatrist gave her their personal cell number to ensure there would be no communication breakdowns.
“They don’t treat mental illness like physical health,” Tracy said. “They don’t use handcuffs if you have a heart attack. They don’t treat mental illness urgently; they lock you up and come see you every couple of days.”
As a result, Tracy remains distrustful of the system, and says she now knows what words to use – and not to use – so she never winds up involuntarily committed again. DRNC heard this from nearly every person with lived experience we interviewed. Research confirms this fear.
“Involuntarily committing people like this state does not prevent suicide. It will just make sure they do it without reaching out for help,” said Bethany,[4] who was involuntarily committed more than 20 years ago and is resolute this will never happen to her again. “Suicidal ideation is part of a lot of mental health diagnoses. It does not mean we will act on it.”
Like Tracy, Bethany works closely with her psychiatrist. But Bethany understands not everyone is as fortunate as she is to have a psychiatrist who “will help me work through my thoughts and not throw my butt in an ED or psych unit.” She worries about people who seek help without understanding what could happen to them. “You need a Miranda warning for mental health,” Bethany said.
Marie, the 11-year-old committed for forced hospitalization, and her parents say she is being treated for Post-Traumatic Stress Disorder (PTSD) related to her experiences in the locked facility. “Not only was she not getting care in there, she was being affirmatively harmed,” Dan said.
Marie was institutionalized during the pandemic and worried she might get sick. The hospital would not allow the patients to wear masks because of the potential danger of ear straps. Indeed, she did get sick and was isolated from other patients, nauseous and vomiting. Her clothes and sheets were soiled, and she said it was hours before hospital staff changed her sheets and provided her with fresh clothing. “It wasn’t just she didn’t get mental health care; she also got sick there,” Megan said.
Then, another sick patient was brought in to be Marie’s roommate in isolation, and while they were in isolation the roommate sexually assaulted her, Marie reported.
Now 15, Marie says those experiences are still with her. “Especially with PTSD, a lot of things bring it back to me. Part of it is, ‘oh, that was a different person, that really didn’t happen to me.’ I did the trauma therapy, and it did help. But it’s still there.”
During the admission process, Marie was strip-searched by a male staff member while a female staff member took notes. “That was one of the most traumatic things,” she said.
Ironically, while the system that was designed to help Marie only traumatized her more, Marie credits her roommates and patients for providing kindness, care, and support. “I had two great roommates. They tried to explain to me what was happening and what to do,” she said. “They really did tell me everything I needed to know.”
Other patients helped her too. “It was people taking care of each other,” she said. “There was one girl there who was 10. I felt very protective of her because she was so young.”
Her roommates showed her additional kindnesses such as sharing their coloring books. Marie said she spent a lot of time journaling and coloring with unsharpened crayons. “I was able to regulate myself and keep out of stuff. I just kept my head down and colored mostly. I was pretty well-liked. There were kids who got beat up, but not me,” she said.
There were fights and yelling, alarms blaring from time to time. She remembers seeing staff holding down kids experiencing panic attacks and administering forced intramuscular psychiatric medications kids and staff called “booty juice” because it is injected in the gluteal muscles. “That was hard,” she said.
Written entries and drawings in her journal reflect her feelings while she was there. “I wanna fucking die. I don’t feel safe in this facility. The staff/kids scare me. I hate it here. Let me go home. Please I wanna go home. Please!”
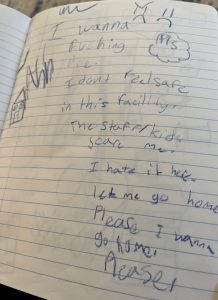
Those sentiments are repeated in various ways throughout her journal. Frowny-faces are prominently depicted. So are drawings of houses, illustrating where Marie wanted to be.
Her journals and drawings demonstrate an extraordinarily difficult time in her life. Still, Marie said she thinks she will keep them “probably forever. It’s helpful when I have to talk to people about it and I can look back at this and it’s evidence. Also, it helps me remember the people I was in with. There’s just something about looking at it and seeing how far I’ve come from then.”
Tracy, Bethany, and Marie shared with DRNC some of the particular harms they experienced in the IVC process. There are additional tolls on people who are committed for involuntary mental health treatment.
“How many of us, if we were picked up and held for 10 days, how many North Carolinians could then pay their next month’s rent? And keep their job?” said Corye Dunn, DRNC’s director public policy. “So, you miss a week of work, then you lose your job, then you lose your apartment, then you’re homeless. So now what? How is that helpful? Who among us could bounce back from that?”
The financial cost of forced hospitalization
Inpatient psychiatric hospitalization is expensive. Whether in a private psychiatric facility, state psychiatric hospital, or community hospital, the cost paid by public programs, insurance companies, and uninsured and underinsured people can run well over $2,000 per day.
Insurance companies negotiate lower rates, but the lowest of those rates in state operated hospitals is $963 per day. That means forced treatment in our state costs hundreds of millions of dollars each year, but limited data, discussed more fully in the data section of this report, makes it impossible to calculate the cost more precisely.
Those charges accrue while a person is hospitalized regardless of whether the person is ultimately committed by a judge. Even under the fastest possible timeline, a person who is taken to an ED on a custody order, assessed quickly, moved efficiently to a 24 hour facility, and after several days in that facility ruled to not meet IVC requirements is likely to incur at least $10,000 of costs, possibly many times more. A 30-day commitment order could easily mean a bill for $60,000. That kind of unplanned expense would derail nearly any household budget.
So, in addition to the legal consequences of an IVC, the lost wages of an unplanned hospitalization, and the trauma potentially associated with forced treatment, people face financial ruin. People who have been forcibly hospitalized frequently ask DRNC attorneys whether they have to pay the bill for the care they didn’t seek or want. Unfortunately, the law says the patient is responsible for the cost even if they didn’t want the treatment.
Medical debt is a widespread problem in NC. In 2024 NC DHHS unveiled its medical debt relief project. But still people with disabilities face the financial burden of treatment under IVC. Kaiser Family Foundation reported that in 2021, 15% of people with disabilities have unpaid medical debt, compared with 6% of their nondisabled peers. IVC poses a serious threat to the financial well-being of people with disabilities.
Like with the trauma, these collateral costs can be significant. “The treatment is worse than the illness,” Bethany said. “I know people who lost everything they own because they don’t have a job because they were locked up in a hospital. This system beats people down. It literally beats people down.”
It is crucial to understand that the people with whom we spoke used their unique strengths and determination to survive their experiences. They are brave to share their stories. They are all focused on the future. They have worked extremely hard to get to where they are today. And they are clear-eyed that their hard work is why they are where they are today, that their hard-won success is not because of the treatment they received through involuntary commitment; they are where they are in spite of it.
For example, when asked, Marie didn’t hesitate to list numerous activities, hobbies, and many friends that bring her joy these days. Her face lights up with she talks about swim team; she describes herself as “a freestyle girl.” Tracy works in IT, volunteers as a guardian ad litem for foster youth, has published a book, and writes an occasional blog. Bethany works as an advocate for people with lived experience.
Recommendations:
- The NCGA, DHHS, and MCOs must increase crisis prevention resources.
- Educate the public, magistrates, and district court judges about the effectiveness of community-based peer support programs as an alternative to IVC.
- Require MCOs and Prepaid Health Plans in Medicaid to ensure the providers in their networks are not just meeting licensure standards but that they are also required to provide evidence-based, culturally competent, and trauma-informed care.
- Amend NC law to require same gender staff to conduct any body searches in psychiatric facilities. Minors should also have a right to have a parent or legally responsible adult of their choosing present during a strip search.
- Amend NC law to require all psychiatric facilities to ensure care is provided in a trauma-informed manner.
- Increase efforts to seek reimbursement for Medicaid payments in cases of abuse or neglect, which, by law, constitutes Medicaid fraud. These funding recovery measures against facilities are a more effective deterrent for abuse and neglect than relying only on licensure actions as is often the case now.
- The DHSR website must provide public access to hospital surveys.
“Nothing about us without us”
On a crisp, sunny morning last December, Cherene Caraco stood before a beautifully-renovated ranch house in Raleigh. The excitement was palpable among the two dozen or so gathered for the ribbon-cutting of Wake County’s first “peer respite” home, called The Retreat @ Fernwood, an unlocked, free, alternative to forced hospitalization and EDs for people experiencing a behavioral health crisis. The respite provides a safe, calming environment staffed 24/7 by trained peer support specialists (PSS), i.e., people with lived experience trained to provide assistance.
“We stand here to open a space where locks, handcuffs, and hard surfaces are being replaced by shared experience, connection, humanity, dignity, and an opportunity to no longer be merely a ‘mental patient,’” said Caraco, CEO of PRN, a peer-led organization that owns and operates The Retreat at Fernwood, and another, Retreat @ The Plaza, in Charlotte. “This is a big deal.”
Caraco is one of NC’s biggest proponents of the necessity and success of peer support services. For years, she and others across the state have strongly advocated for the development and expansion of peer-led support services, which research has strongly shown are effective ways to promote mental health and substance use recovery, as well as prevent costly psychiatric hospitalizations.
NC DHHS is now promoting the value of peer support in a variety of ways, including expanding PRN’s Charlotte-based “peer warmline” to a free statewide, peer-run service available 24/7 for people in crisis. People can call the number any time and speak with someone who understands their experience. In May, DHHS released a dashboard that tracks the warmline’s work, reflecting a 100 percent satisfaction rate among the more than 67,000 callers between April 2024 and March 2025 who completed a survey.
Director Crosbie spoke at the ribbon cutting about how peer support helped her father and other family members, including her. “Peers are amazing. I’m talking to a group that understands that already, but not everybody does. So often with other groups, I talk about all the research, the study after study after study that talks about the effectiveness of peers, but just from a real human perspective, peers were life changing for me. They were the only thing that ever helped my dad feel better for a few minutes, which really helped me, helped his family, which was a big deal for us.”
Like The Retreat @ The Plaza in Charlotte, The Retreat @ Fernwood is beautifully furnished and welcoming, a far cry from the sterile and stiff interiors of psychiatric hospitals and EDs. Each room invites the visitor to relax and feel safe. The staff, all peers, are understanding and affirming.
The stay is free and can last up to seven days. PRN has plans to open another retreat, in Cabarrus County.
“What tried to kill me I use to help other people,” said Sharon Galusky, a PSS at PRN in Charlotte, in describing how she helps people in their healing journeys. PSS are essential to recovery as they play critical roles in advocacy, resource sharing, building skills, community and relationships.
PSS are also adept at leading recovery groups, mentoring, and setting goals for people on their journeys to mental health wellness. As a primary goal of PSS is to help achieve recovery from mental health crises, strategic placement of PSS in critical positions within an organization maximizes benefit to the organization as well as recovery of people served.
In 2022, DHHS awarded nearly $4 million to increase certified PSS across eight community-based organizations focused on substance use recovery. At the time of the award, there were over 4,000 certified PSS in NC. As part of its focus on PSS, DHHS offers a certification program as well as scholarships to participate in the program.
Psychiatric survivors across the country have been grappling with Illness-based mental health systems for years and have important, informed recommendations for improving mental health outcomes through recovery-based models. The best way to honor their experiences is to include them as we are making policy in NC. This report provides additional information on non-coercive mental health practices.
The peer movement shows how effective approaches can be when disabled people are involved and actually lead efforts. “Nothing about us without us,” is a mantra often cited by the disability community. Peer-led supports and recovery shine as examples of why that is true.
More innovative approaches
Promise Resource Network – Charlotte
In addition to PRN’s retreats and warmline, DRNC’s investigation revealed additional dynamic practices have given rise to effective and sustainable utilization of resources centered on meeting behavioral health demands in the community, both for people in recovery for mental health and/or substance use.
These approaches place service in the hands of people who are uniquely equipped to fill behavioral health needs instead of taxing law enforcement and EDs to perform tasks they are not adapted to field. Developing an increased awareness and broader understanding of the value of these practices can lead to widespread implementation across the state and improve outcomes for law enforcement, EDs and the communities they serve.
PRN in Charlotte began with a wellness center, , that now offers over 55 classes each month, in-person, virtual and hybrid, all centered on wellness at no cost to people in recovery.
The Hub is open access and requires no referral. The Hub offers classes for practical skills and creative outlets, employment placement and support, street outreach, shelter and housing support, court and diversion support that advocates for court involved participants and provides training to criminal justice professionals as well as re-entry support for people released from jail. PRN is one of the most innovative community providers as it also offers the PRN Incubator: supporting emerging leaders in recovery. PRN’s Recovery Café uses a membership model in promoting a healing recovery community within the Recovery Hub building.
And it continues to expand. “When people are being seen and heard, they show up,” Caraco said.”
“Everybody here is guaranteed love, acceptance, and respect,” said Galusky.
Bobby Livingston, a PSS who had been involuntarily committed more than 30 times, sometimes as many as three times a month, worked at PRN until he recently retired. After finding PRN, Livingston was not hospitalized again, and owns his home and several cars. He loves his cars, joked Caraco. He participated in a panel discussion about the IVC process at DRNC’s 2024 conference.
“People aren’t taught about recovery,” Livingston said, noting that recovery and the existence of peer support bring people back to life. “We don’t put out the fire, we start it,” he proudly said.
Caraco echoed that idea. “Instead of person-centered planning, it should be dream-centered planning. Because in this system you lose your dream, you are reduced to nothing but your label, your diagnosis. We need to be hope dealers, dealers in hope.”
In addition to continuing to champion peer-supported services and organizations in NC, Caraco recently traveled to Trieste, Italy, with a group of mental health advocates and clinicians from across the United States to explore how that community has nearly eliminated forced psychiatric treatment. The Trieste model relies almost exclusively on care and services in the community and especially in homes.
Already well-rooted in recovery as a way of life, Caraco returned from Italy with a deeper understanding of recovery and inclusion and said, “fostering recovery and social inclusion means that recovery isn’t a question, a model, or a practice. It is a truth and way of being with one another. Social inclusion means social cooperatives, community living, and deep relationships.”
“Why do you spend so much money on buildings?” Caraco said someone in Italy asked the group of American delegates. “Crisis services should be provided in homes, not mental health centers,” she said. Now she is looking to develop a pilot program in NC that would be situated with PRN using some of the elements the delegation saw in Trieste
The Trieste model focuses on five core values:
- Helping the person, not treating an illness
- Fostering recovery and social inclusion
- Addressing the person’s needs that matter to the person
- Respecting the person as a citizen with rights
- Changing the attitude in and of the community
“Everything is relationship-based. It is all psychological safety and relationships,” Caraco said.
GreenTree – Winston-Salem
“I wish there were a place where people like me—people whose minds work differently—could just talk and be people together.” These were the words of Laurie Coker’s son, Peter, when he was about 15 years old. Peter died by suicide in 2009 at the age of 27.
In 2012, Coker, a retired psychiatric nurse and staunch mental health advocate, was inspired by Peter’s words and life to found GreenTree, a peer-developed and operated social and wellness hub in Winston-Salem.
GreenTree was born in a church-owned building that was empty during the weekdays. The church allowed the peer center to operate there at no cost for 10 years “because it so much believed that this healing space was needed in our community,” Coker said. In recent years, a state Peer Run Wellness Center Grant allowed GreenTree to start paying rent.
“We’re not just peer-driven, but also community-driven. The county is very supportive,” Coker said. “We’ve seen so many wonderful changes in people’s lives, and this has been clear to county leadership and advocates.”
Coker says having a community space like GreenTree is crucial to mental health and substance use recovery. “We all need space for community connections where we can have the emotional safety to exhale and find soul validation. Too often, people do not receive such validation in our mental health systems,” she said.

GreenTree’s grounds include a store front building with a sitting area furnished with café tables and chairs, a reception counter, coffee and snacks. There are rooms dedicated to learning and groups, and rooms that accommodate larger numbers of people for trainings. Outside there is a garden with flowers and vegetables where participants learn about healthy eating habits and growing their own food.
GreenTree is a welcoming space for people who live with mental health extremes. This peer-run organization offers wellness through group activities, creative arts, peer to peer support, including a new program for youth peer support, and practical support like getting help with eyeglasses, scheduling appointments, and connecting people with the resources they need. GreenTree offers healthy cooking classes and other educational opportunities as well as trainings for law enforcement and other community members within its welcoming space.
GreenTree partners with community agencies to create a safer space outside its walls as well. For example, local law enforcement is aware of the organization and its offerings and will divert people in crisis to GreenTree instead of a hospital ED or jail. Coker partners with local hospitals to ensure people who are discharged and experiencing homelessness have a safe place to go. Hospital staff contact GreenTree so a PSS can pick up the person in need and bring them to the safety of GreenTree’s Refuge House, day or night.
Refuge House is a safe, quiet home that allows for comfort, privacy, food, a washer/dryer and other comforts of home. This safe space creates a buffer between an individual and the debilitating stress he or she may be under. Further, the peer staff determine from guests how they can assist them in getting services or treatment they desire but find challenging to access on their own.
The stays are for 24 hours at a time and can mean the difference between an IVC or jail. “Just to be able to be safe and rest for 24 hours can help a lot,” said Michael Alexander, a PSS for GreenTree. “It doesn’t look clinical, and people can rest, take a nice shower, and have something to eat.”
Often people who come to Refuge House begin to participate in activities in the hub, even if it is only to have coffee and sit quietly. Coker strongly believes inclusion in a community is healing.
As she reflects on GreenTree, Coker thinks about Peter. “I keep thinking, what if Peter had had a place like this in his life?”
Jubilee Healing Farm – Hillsborough

Founder Dr. Nora Dennis is a psychiatrist who spent years helping people access mental health services in a corporate setting. A few years ago, she was drawn to focus on healing in a different way and purchased 10 acres of land that is now Jubilee Healing Farm in Hillsborough.
The farm has a variety of gardens with many plants, trees, and bushes that provide fruit, vegetables, and herbs that participants can cook in the full kitchen in the main building. Also inside the building is a space with sofas and chairs for comfortable seating, and an area that is open for yoga, meditation, or dance. The entire building is open and inviting with abundant natural light.
“Dr. Nora,” as she is known, has a soft voice and an easy manner that invites safety and conversation. She says the program employs a medical model involving treatment plans, medication management, and therapy, and adds in movement, cooking, and the outdoors.
“It feels more holistic, and having mindfulness is an important part of our work and model,” she said. “I wanted to create a program I would feel comfortable sending my family to.”

A small cabin serves as an inviting space for individual therapy, with views of the farm and a fenced area for curious, friendly goats. Not far away is a large white permanent tent for multiple uses, as well as a huge, inviting hammock under a canopy of trees and shade.
And there are long-haired bunnies in an outdoor hutch next to an enclosed circle of hay bales that serve as a site for group therapy. are allowed in the circle during group so people can hold and pet the bunnies while they are there.
Dr. Nora’s family dog, a shy, sweet rescue pup named Winnie, has free roam of the place
Staff at Jubilee Healing Farm provide multi-disciplinary, team-based behavioral health care that includes a therapist, psychiatrist, and PSS who collaborate to support individual well-being. They provide intensive outpatient and partial hospitalization programs as well as medication management and outpatient therapy.

Jubilee Healing Farm is unique in its convergence of western medicine techniques with holistic approaches, creating a healing space with five values: community, presence, ecology, balance, and radical honesty. While the focus is on evidence-based clinical care, it also provides a client-centered holistic approach focused on self-care. There is a reliance on nature and animals to achieve healing. Jubilee rotates guest presenters to offer topics including earth skills, art, herbalism and cooking. And they invite the community to help tend the garden and be a part of the community through participation in workshops open to everyone.
Holistic Empathetic Assistance Response Team (HEART) – Durham
The City of Durham has launched a highly promising initiative that is the first of its kind in NC. The Durham Community Safety Department (DCSD) works alongside the Durham Police Department using four teams reliant upon mental health/medic/police partnered responses in serving the city. In June 2022, the DCSD launched the innovative Holistic Empathetic Assistance Response Team (HEART) to meet community needs that typical police responses did not fulfill. The program has been operating citywide in Durham since October 23, 2023.
HEART was created in response to the community’s demand to rethink policing following George Floyd’s murder. Originally a pilot program sprung from community efforts, nearly three years in HEART is described as a “beacon of hope for Durham residents.”
HEART is a highly effective non-police response to crisis calls. It diverts mental health related calls from unnecessary ED visits and frees law enforcement to fill law enforcement duties. HEART matches the needs of people in crisis with appropriate existing services. Services are offered from the initial call for help and continue as needed until the person is connected with community resources to address the person’s needs. This connection to community-based care ensures access to resources and heads off future crises.
HEART is comprised of four distinct teams that work together to meet the demands of the community by phone and in the field.
HEART Crisis Call Diversion Teams (CCD) are mental health clinicians embedded in 9-1-1 call centers who immediately respond to behavioral health crises while also offering support to 9-1-1 dispatchers and first responders in the field. CCD counselors are able to resolve some crises over the phone through provision of resources and elevate the remaining callers to other HEART teams. To ensure callers’ needs have been met, CCD counselors check in after contacts to ensure callers are able to access needed services.
Community Response Teams (CRT) are first responders called to non-violent mental health crises that include mental health clinicians, PSS and EMTs. The Co-Response Team (CoR) pairs mental health clinicians with Crisis Intervention Trained police officers for calls that may pose a safety risk. Finally, Care Navigation (CN), comprised of mental health clinicians and PSS follow up in person or by phone for additional support and ensure the community member is aware of available community resources following responder intervention. Durham is the first city in NC to enlist CCD and CRT teams.
HEART’s online dashboard data is transparent and comprehensive. Between June 2022 through early May 2025, HEART’s CRT diverted 12,729 calls from Durham Police Department. The average time to complete a call is under 50 minutes for CRT and just over an hour for CoR. Since its launch, until early May 2025, HEART has responded to 30,199 calls with police backup called for team safety only .02% or just under six times, indicating HEART responders navigate their duties in safety.
HEART responders report feeling safe in 99% of encounters. This is a tremendous savings measure as the financial cost of police first responders for people in mental health and substance use crises is more than four times greater than a community response model.
HEART is a powerful community response answering the call of its citizens. It is seeking to expand its operations to run 24/7. It offers a promising alternative to police response that is favored by its community. To understand HEART’s impact on the community, consider the words of a member of the community quoted in a recent article in INDY Week: “Whenever I see the HEART vans driving down the street and I’m with my kiddos, they’re like celebrities to us.”
Recommendations:
- Invest in more non-coercive, non-law enforcement approaches to mental health crisis, such as the HEART model.
- Make community-based care readily available to prevent crisis.
- Include and listen to people with lived experience in designing services and supports.
- Expand peer support throughout the service system.
NC has made IVC far too easy
Over time, incremental policy changes have increased overreliance on IVC at the expense of personal liberty and community mental health services. These changes have broadened IVC criteria, relaxed requirements for IVC examinations, and weakened judicial due process protections in favor of the judgment of physicians and mental health professionals, even though unjustified segregation of individuals with disabilities constitutes discrimination under the Americans with Disabilities Act.
In 1973, NC enacted legislation to ensure that individuals could only be involuntarily committed to a mental health facility if they were:
- “Mentally ill or an inebriate” AND
- Imminently dangerous to themselves or others
NC policy protected individuals’ dignity and constitutional rights, ensuring that IVC was a last resort and that individuals were discharged as soon as a less restrictive mode of treatment was appropriate. “Dangerous” meant harm would have to occur in the immediate future. This was a change from caselaw that required an actual attempt to harm for someone to be “dangerous.”
Today, the criteria for involuntary commitment in NC require:
- Mental illness AND
- Dangerousness to self or others
The word “imminently” was removed.
Through the years the definition of “danger to self” has broadly expanded to include attempts, threats, and even probability of self-mutilation or suicide and an inability to meet basic needs, like food and shelter, that will likely lead to physical debilitation in the near future. “Danger to others” means attempts, threats or actual harm to others as well as extreme destruction of property. The expanded definitions have made IVCs more commonplace.
Over time, incremental changes in policy have had a significant impact on the IVC process. Removing the “imminent” danger requirement and expanding who can serve as first commitment examiners cast a wide net for involuntary commitment.
In addition, NC’s law used to require in-person examinations “so that the physician may actually utilize his five senses… in carrying out the mandate of the statute… To hold otherwise would increase the possibility that persons who are not mentally ill or inebriates and dangerous to themselves or others would be involuntarily committed.”[5]
Now first examinations happen via telehealth if the examiner is “satisfied to a reasonable medical certainty” the outcome would be the same if the exam happened face to face. While these changes aim to provide timely care, they also raise concerns about the potential for unnecessary forced hospitalization.
The IVC process must conform to the Fourteenth Amendment that prevents states from depriving people of liberty without due process of law. Due process guarantees the right to be notified of an action that would take away a person’s liberty, and the right to a hearing in front of an impartial judge.
In addressing due process in the context of IVC, the Court of Appeals attempted to strike a balance with forced treatment and the law. The court ruled that the requirements of two commitment examinations and a hearing within 10 days of initial detainment adequately ensure a respondent is not being [6]
However, in 2009 a change in NC law allowed successive 7-day petitions, disrupting the balance of IVC due process. While the statute requires each successive petition to be based on an updated assessment, our investigation revealed, as in Ben’s case, that is not always what happens. Additionally there is no limit on the number of successive petitions in a single ED admission. When repetitive petitions occur the situation is particularly problematic because no judicial oversight is guaranteed and legal counsel is not assigned to people in EDs. Effectively, the individual’s right to liberty is decided by a physician based on clinical impressions, not an impartial judge sworn to uphold Constitutional due process.
While physicians should release a respondent as soon as criteria for IVC is no longer met, our investigation revealed a lack of adherence to that obligation. Instead, an admission may continue for the length of time approved by insurance regardless of the legal status of the respondent.
The 10-day hearing is the final step in the IVC process and the step that guarantees due process. This hearing is critical for more reasons than a judge’s determination of discharge or ongoing treatment. A commitment leads to lifelong consequences: not only the loss of rights and privileges discussed throughout this report, but also the fact that prior IVCs, petitions, orders and evaluations can be used as evidence in future commitment hearings.
The standard of proof at a commitment hearing is clear, cogent and convincing, which is lower than beyond a reasonable doubt.[7] While the State can deprive people of liberty through IVC, it can only do so if the State or 24-hour facility prove by clear, cogent, and convincing evidence that a respondent is mentally ill and dangerous to self or others.[8]
Even with this standard of proof and the acknowledgment that IVC is a “significant curtailment of liberty requiring due process protection,”[9] respondents are being committed to privately-owned 24-hour facilities that are not required to have attorneys at commitment hearings to present evidence to meet that standard of proof[10]. This requires judges to pose questions and examine witnesses, rather than remaining as a neutral decision-maker who has both sides presented to them.
It is unclear how many judges at the 10-day hearings adhere to the standard of clear, cogent, and convincing evidence in order to extend a person’s hospitalization. In Marie’s situation, that standard certainly was not met.
Dan recalled the virtual hearing he and Megan attended on Marie’s behalf. The question before the judge then was whether he would allow Marie to be discharged or require her to remain confined to the facility for up to 15 more days.
Marie’s lawyer, known as “special counsel,” had spoken with Megan and Dan in advance of the hearing and told them she thought it best if they spoke to the judge about Marie and the significant outpatient plan they had lined up for their daughter.
Dan followed that advice. Then the judge turned to the hospital’s representative for their position. Dan said he couldn’t believe what he heard. “Fifteen days,” is all the doctor said, Dan reported. The facility presented no evidence about how Marie was doing at the facility, and if clinicians there felt she needed additional hospitalization, why.
And with that, the judge indicated he was prepared to commit their daughter for another 15 days, even after they told the judge they had extensive treatment plans ready for her back home and how frightened Marie was there.
Dan fell back on his experience as an attorney and asked the judge not to do that. He said Marie’s plans were already scheduled and wouldn’t work out if she couldn’t begin the treatment right away.
They were relieved that the judge then changed his mind and ordered Marie’s release. But Megan and Dan remain incredulous that with only two words, “fifteen days,” the judge was prepared to force Marie to remain in the facility for 15 more days.
“Fifteen days?!” Dan said. “They were throwing her to the wolves. That they could do that and would do that? The system is cooked to do this to our kids.”
Marie recalled learning she was leaving. “I remember being shocked because they said you are going home, and I was so happy,” she said.
After her parents picked up Marie, the three drove to the beach and spent the night at a friend’s house, where they could breathe salt air and feel the sand. “I was so relieved to get her out of there,” Megan said.
Still, Megan and Dan worry about children whose parents or legal guardians may not have the means and education to advocate for their children against a system they see as stacked against kids. Many adults who have experienced the IVC process feel it is stacked against them, too.
The evolution of NC’s IVC process reflects a shift towards broader legal criteria for forced treatment. While the intent has been to provide timely care to those in need, that is not what has happened. Rather than building an effective community-based service network to address the cause of the mental health crisis, NC broadened the criteria for commitment, expanded the numbers of commitment examiners, and permitted detention of individuals indefinitely without judicial oversight. This long-standing problem of trying to address shortages in the mental health system with procedural changes in the law violates rights, creates significant and lasting harm and is an inefficient and wasteful use of resources.
Recommendations:
- Shorten the time to a judicial hearing from ten days to five days from the beginning of custody or three days from arrival at 24-hour facility, whichever comes first.
- Allow and facilitate attendance by minor children’s parents and guardians at all judicial hearings.
- The NCGA should clarify in statute that privately-owned IVC-receiving facilities are required to be represented by an attorney at judicial hearings just like NC’s state-operated facilities.
Full 2025 Recommendations to reform the NC Involuntary Commitment Process
- END MISUSE AND OVERUSE OF IVC
- Require an in-person screening by a local mobile crisis team before a custody order can be entered. This would help identify bad actors seeking to IVC someone for inappropriate purposes. It also helps to identify whether IVC is appropriate before anyone loses their liberty.
- Amend NC law to require that IVC petitions of children and adults under guardianship include information about parent/guardian’s involvement in seeking and planning care and reasons why voluntary treatment could not meet the respondent’s needs.
- Require specialized training for magistrates on the use of the IVC process. This training must include the collateral costs of IVC, the trauma IVC causes, and the benefits of NC DHHS’s crisis services information, including access to Peer Warmline, 988, peer support, and trauma-informed recovery models.
- Amend the prerequisites for custody orders by including a requirement that the magistrate first affirm the following:
- Petitioner has taken steps to avoid IVC, including suggesting calling the peer warmline or 988, or enlisting other crisis resources
- Magistrate has considered and balanced the social costs of IVC, including time out of work or school, stigma, medical costs, and trauma. If the facts, as alleged, are true, would any benefit of the commitment outweigh the likely costs?
- Magistrate has considered and inquired into the motivation behind the petitioner, including possible misuse of IVC
- Magistrate has inquired whether respondent has an Advance Instruction for Mental
Health Treatment, also known as a Psychiatric Directive (PAD), and if there is one, that it is being followed.
- Create a study of feasibility of hospital treatment cost-shifting to petitioners to deter the practice of frivolous or repeated IVC that is later found to have been unnecessary. This would address the practice of some Adult Care Homes and Skilled Nursing Facilities to misuse IVC as a legal mechanism to move residents off their caseload.
- REDUCE HARM DURING TRANSPORT
- Require facility providers to notify the respondent and their parents, legal guardians, and/or family members, about the option to transport the child or adult themselves. This should be done verbally and in writing.
- When transport by family is not possible, reduce trauma and stigma during transport by amending NC law and Medicaid policy to require public and private insurance companies, MCOs, and Medicaid to fund and enter transport agreements with appropriate non-law enforcement providers to transport people to and from available inpatient mental health facilities in a trauma-informed manner.
- Require all transporters to be trained in and utilize trauma-informed approaches.
- For law enforcement transport, prohibit the use of shackles or in the alternative, require a law enforcement officer to obtain prior authorization from a commanding officer and file a report (reasons and outcome) when handcuffs or shackles are used. Prohibit or discourage the use of marked cars and uniformed officers and encourage same-gender officers when possible.
- REDUCE HARM IN FACILITIES AND COURT
- For minors, give their parent or a legally responsible adult of their choosing the right to be present during a strip search.
- Amend NC law to require same gender staff to conduct any body searches in psychiatric facilities.
- Require that emergency hospital staff and psychiatric facility staff assigned to care for people under custody orders have training in and utilize trauma-informed approaches.
- Allow and facilitate attendance by minor children’s parents and guardians at all judicial hearings.
- When parents, legal guardians, and caregivers are supportive, include them in communications and medical decisions in EDs and in 24-hour facilities.
- To reduce time in custody for people who may not need it, amend NC law to eliminate successive petitions.
- Expedite the judicial hearing by reducing the time from ten days to five days from the beginning of custody or three days from arrival at a 24-hour facility, whichever comes first.
- Amend NC law to appoint special counsel or contracted appointed counsel at the time magistrate issues the custody order so respondents can have timely representation. This provision will require funding for additional staff.
- Deter facility-based abuse and neglect by Medicaid providers by increasing efforts to recover Medicaid funds in cases of abuse or neglect in addition to facility licensure penalties.
- Clarify in legislation that privately-owned IVC-receiving facilities are required to be represented by an attorney at judicial hearings just like NC’s state-operated facilities.
- BUILD OUT EVIDENCE-BASED ALTERNATIVES
- Fund additional community-based care and make it readily available to prevent crisis.
- Fund more non-coercive, non-law enforcement approaches to mental health crises, such as the HEART model in Durham.
- Require MCOs and Prepaid Health Plans in Medicaid to ensure the providers in their networks are not just meeting licensure standards but are also required to provide evidence-based, culturally competent, and trauma-informed
- Include and listen to people with lived experience in designing services and supports.
- Expand peer support throughout the service system.
- COLLECT AND SHARE DATA
- Require collaborated reporting by AOC and DHHS of the following key data:
- Category of the petitioner, i.e., law enforcement, family member, domestic partner, clinician, other, for each petition sought.
- Race, age, ethnicity, and gender for each respondent.
- Outcome of each petition, dismissal or custody order granted.
- Transport method to the ED or other site of first evaluation for people under a custody order for IVC.
- Number of people discharged from an ED after a custody order because they didn’t meet the legal criteria for commitment following the first evaluation.
- Number of successive 7-day petitions per hospital as well as per respondent.
- Number of people transported to 24-hour facilities, specified by facility of origin.
- Number of people transported to 24-hour facilities from EDs.
- Number of people discharged from 24-hour facilities prior to the 10-day IVC commitment hearing, broken out by day of stay, i.e. discharged on Day 2, or Discharged on Day 9.
- Number of people discharged from 24-hour facilities at the 10-day hearing.
- Lengths of stay (LOS) for children and adults in EDs under IVC proceedings.
- Make all data related to the use of the IVC process readily available to policy makers and the public on an electronic dashboard.
- Require DHHS (DHSR) to publish hospital surveys on its website so the public can see the regulatory history of the facilities.
- Educate the public, magistrates, and district court judges about the effectiveness of community-based peer support programs as an alternative to IVC.
References
[1] DRNC is North Carolina’s federally-mandated Protection and Advocacy (P&A) organization, one of 57 P&As across the country, charged by Congress with advocating for the legal rights of people with disabilities statewide. DRNC is the only organization in North Carolina dedicated to advancing and defending the rights of all people with disabilities, of all ages, statewide.
DRNC’s mandate includes federal authority to monitor in settings where disabled people receive services to ensure their rights are protected and people are free from abuse, discrimination and neglect. DRNC staff used this monitoring authority to monitor in the EDs we selected.
[2] Ben is not his real name. DRNC is using this pseudonym to protect his privacy. Ben will appear again in the Transportation section of this report.
[3] This is the same person who was committed to a psychiatric hospital based on a blank petition.
[4] Bethany is not her real name. DRNC is using this pseudonym to protect her privacy.
[5] McLean v. Sale, 54 N.C. App. 538, 542-43 (1981).
[6] In re: Zollicoffer, 165 N.C. App. 462, 468 (2004).
[7]In re: Nowell, 293 N.C. 235, 247 (1977).
[8] Addington v. Texas, 441 U.S. 418, 433 (1979).
[9] In re J.R., 383 N.C. 273 (2022).
[10] This differs from what is required in state-operated facilities, which are required under North Carolina law to have attorneys to represent the facility at these hearings.
[11] Indiana v. Edwards, 554 U.S. 164, 178 (2008).
Report Resources